
Inside the Process: Turning Clinical Research into Clean Content
As an MD, I know how much work goes into the science. As an editor, I know how much work goes into the story. This case study shows my full workflow for ” Lifestyle Medicine” from coding the multi-angle shots to designing the motion graphics. If you’ve ever wondered how a raw script becomes a polished final export, this is for you.
Phase 1: The Blueprint (Research & Strategy)
Finding the Gap
We already know the clinical side, but what are patients actually typing into the search bar? I dig into the competitor landscape to find out where other creators are getting the science wrong, giving us the perfect angle to step in as the actual authority.
For example, in this lifestyle medicine project, the gap was glaring: the algorithm was flooded with fitness gurus pushing the oversimplified “eat less, move more” mantra, completely ignoring the metabolic roadblocks our bodies actually build against us.
Finding massive oversights like that gives us the perfect angle to step in as the actual authority and explain the real physiology behind the struggle.
Prep for SEO
Even the best clinical advice is useless if no one sees it. I handle the backend SEO, translating our heavy medical terminology into the exact phrases patients are actually typing into search bars. This bridges the gap between the science and the algorithm, pushing your content right past the fitness influencers.
In this specific script, we dive deep into the 6 pillars of Lifestyle Medicine, specifically how cortisol affects belly fat and how sleep deprivation spikes ghrelin. But patients don’t search for “hypercortisolemia” or “ghrelin dysregulation.” They search for answers to their frustration. Here is how I mapped the metadata to match what people actually type:
What the Textbooks Say
Sleep-induced Ghrelin/Leptin imbalance
Cortisol-induced visceral fat storage
The 6 Pillars of Lifestyle Medicine
Environmental determinants of obesity
What the Audience Searches
“Why am I always hungry at night?”
“Why stress makes you gain belly fat”
“Eat less move more not working”
“How to fix metabolism naturally”
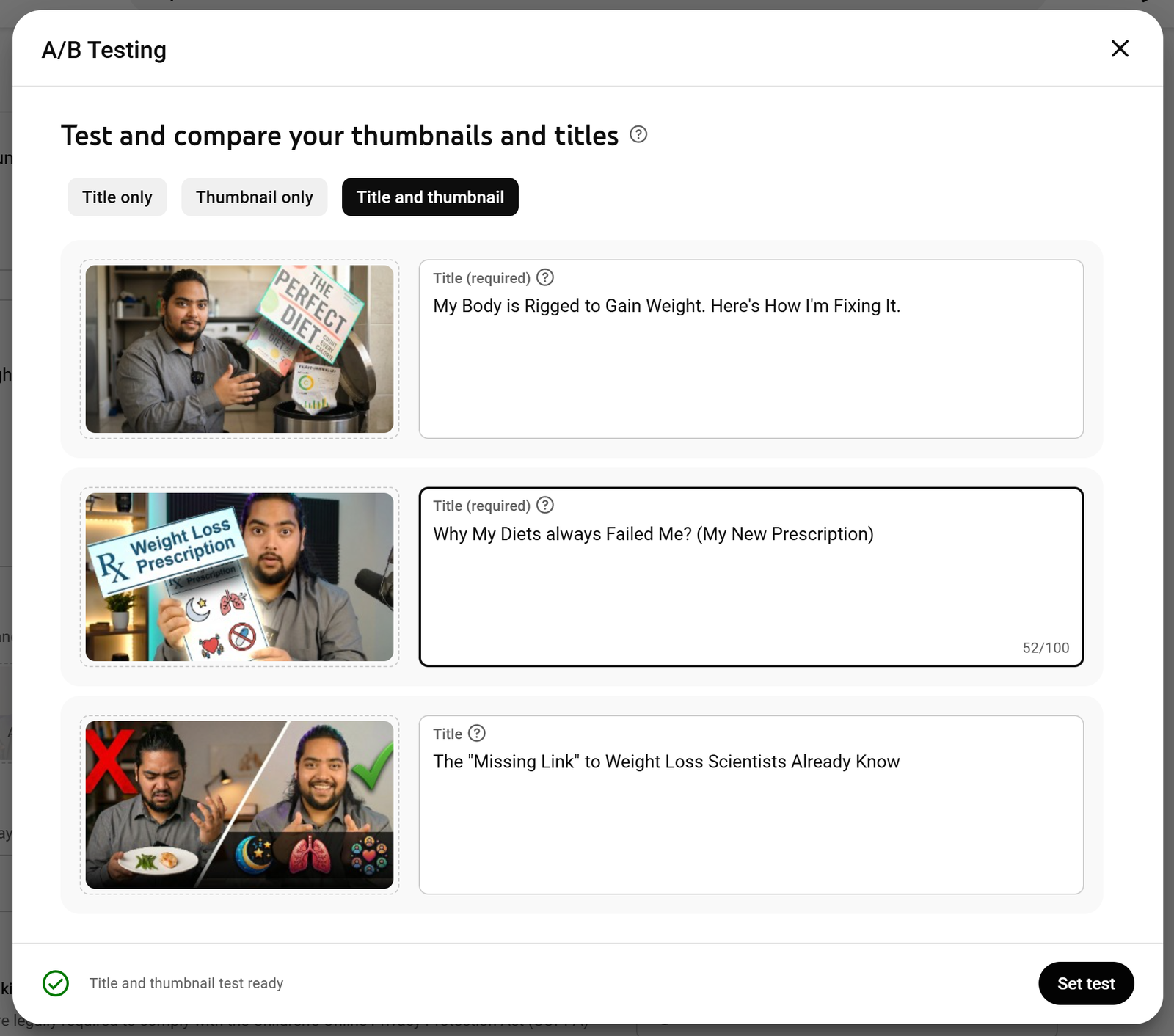
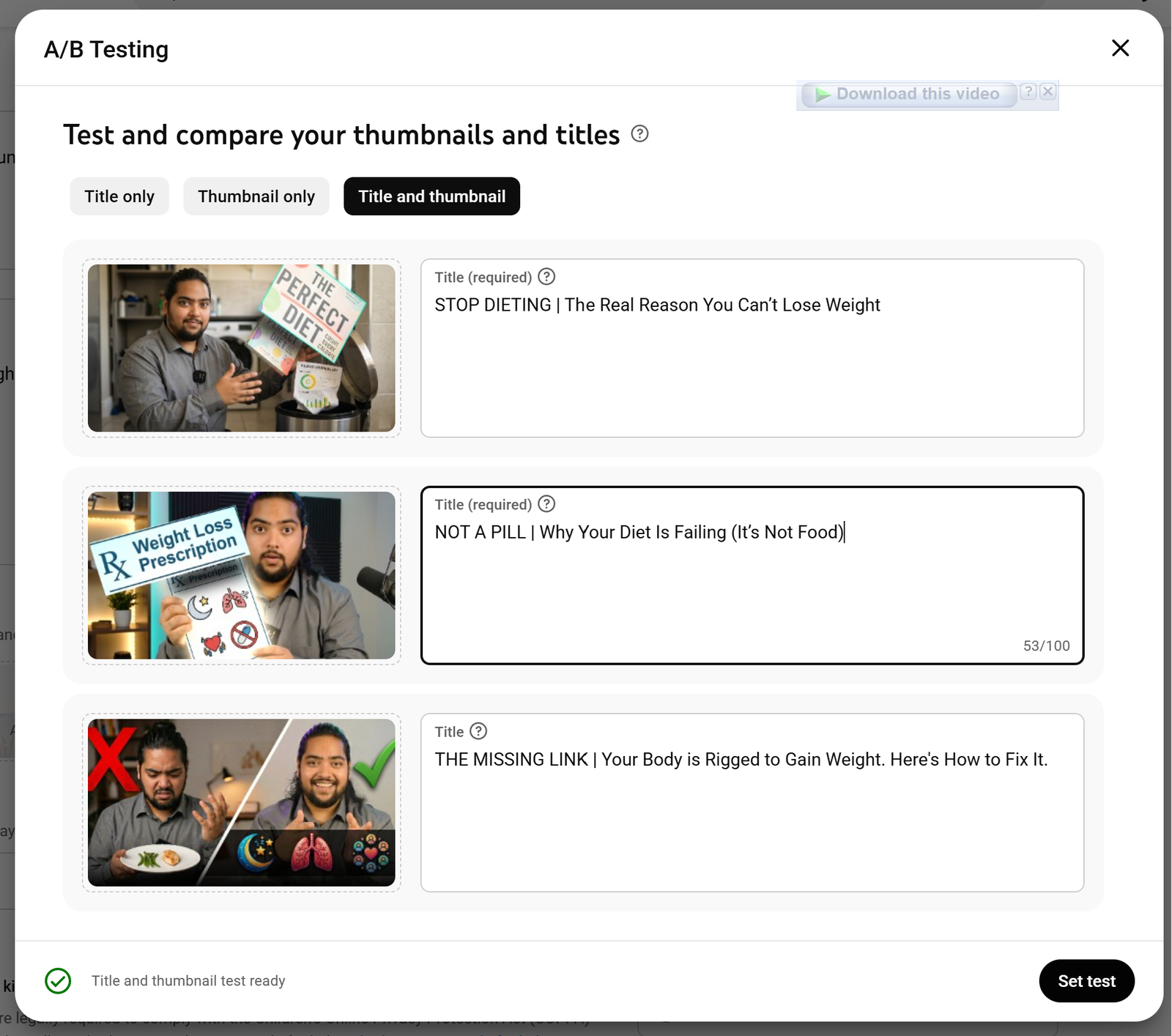
Packaging the Pitch (Thumbnails & Titles)
You can have the best medical advice in the world, but if the packaging is boring, no one clicks. I’ll show you the three thumbnail and title variations I tested to find that sweet spot: highly clickable, but zero cheap clickbait.
Phase 2: Literature Research & Transformation (AI Integrated)
Doing the actual research
Every project starts with a frustration. I was tired of the “just eat less” advice that ignores how our biology actually works. As an MD, I knew there was more to the story, so I went back to the clinical papers to find the “why” behind the struggle. This is the messy part, the raw research notes and the initial brain-dump where I bridge the gap between medical journals and a script that actually makes sense to a human being.
1. “Metabolic adaptation to weight loss: implications for the athlete” (Trexler et al., 2014)
This review details “adaptive thermogenesis.” It explains that during caloric restriction, total daily energy expenditure (TDEE) and basal metabolic rate (BMR) decrease disproportionately to the actual loss of metabolically active tissue. This suppression is driven by changes in mitochondrial efficiency and circulating hormones, intentionally slowing weight loss to prevent starvation.
2. “Persistent metabolic adaptation 6 years after The Biggest Loser competition” (Fothergill et al., 2016)
A landmark longitudinal study demonstrating the permanence of metabolic slowing. Researchers found that subjects’ resting metabolic rates remained ~500 kcal/day lower than expected six years after their initial weight loss, even after substantial weight regain. This confirms that metabolic adaptation is a persistent biological attempt to defend a previous physiological “set point.”
3. “Optimal Diet Strategies for Weight Loss and Weight Loss Maintenance” (Kim, 2021)
This paper directly challenges the traditional “eat less, move more” dietary model. It highlights that energy intake and expenditure are intrinsically linked; interventions aimed at creating a deficit trigger immediate physiological adaptations that actively resist further weight loss, rendering static calorie-counting formulas inaccurate over time.
4. “Metabolic Consequences of Weight Reduction” (StatPearls, 2023)
A comprehensive biochemical overview of how weight reduction alters baseline metabolism. The text quantifies that BMR decreases by approximately 0.02 kcal/min for every 1% decrease in body weight, shifting the individual’s baseline energy requirements downward and necessitating continuous recalculation of caloric deficits.
5. “Physiology, Obesity Neurohormonal Appetite And Satiety Control” (StatPearls, 2022)
This chapter maps the hypothalamic integration of peripheral signals. It details how the body regulates energy homeostasis through the precise balance of ghrelin (stimulating the lateral hypothalamus for hunger) and leptin (stimulating the ventromedial region for satiety). Caloric restriction disrupts this balance, persistently elevating ghrelin and suppressing leptin.
6. “Appetite Regulation: Hormones, Peptides, and Neurotransmitters and Their Role in Obesity” (Klok et al., 2019)
This article examines the role of gut peptides and the vagal nerve in nutrient sensing. It explains that a caloric deficit triggers the hypothalamus to synthesize Neuropeptide Y (NPY) and Agouti-Related Peptide (AgRP), which acutely and aggressively increase the biological drive for food intake, overpowering conscious dietary restraint.
7. “Psychological considerations for the holistic management of obesity” (Zainal et al., 2023)
This paper explores the bidirectional relationship between obesity, weight stigma, and mental health. It outlines how the physiological stress of chronic dietary restriction is linked to cortisol regulation and emotionally driven eating, demonstrating that biological stress directly sabotages behavioral adherence.
8. “An Overview of Factors Associated with Adherence to Lifestyle Modification Programs…” (Burgess et al., 2017)
An analysis of why clinical adherence to diet and exercise protocols universally declines over time. The study identifies systemic psychological barriers, noting that chronic stress, body shape concern, and clinical depression are primary predictive factors of attrition, rather than a simple lack of willpower.
9. “Enough with simplifying: ‘eat less and move more’: at what point are we with the treatment of excess weight…” (Maffeis et al., 2024)
A critique of the medical community’s reliance on simplistic behavioral advice. It categorizes the predisposing factors of obesity into polygenetic effects, epigenetic inheritance, and obesogenic environments, concluding that prescribing simple calorie reduction ignores the multifactorial etiology of the disease.
10. “Stakeholder Input – Semaglutide (Wegovy)” (CADTH, 2022)
While a clinical review of pharmacology, this document outlines the clinical consensus regarding lifestyle modifications. It confirms that instructing patients to independently manage a highly complex metabolic disease solely through dietary math increases psychological stigma and fundamentally misunderstands the physiological difficulty of sustained weight loss.
Raw Notes: The “Eat Less, Move More” Myth
Okay, so here is where the whole video concept started. I was just getting so sick of online gurus and honestly, even standard clinical advice sometimes just telling people to “eat less and move more.” Like, thanks, obviously. We all know the basic physics of it. But if it’s that simple, why can’t we just do it? I’ve experienced this disconnect myself, so I figured there has to be a deeper physiological reason. I dug into the literature, and it turns out, our bodies actively fight against us when we try to lose weight.
Here is the initial brain-dump of the papers I pulled. Need to translate these into normal English for the script.
The Metabolism Trap:
Found this paper by Trexler et al. (2014) talking about “adaptive thermogenesis.” Basically, when you cut calories, your body panics. It slows down your metabolism way more than it should just to stop you from starving.
Then there is the Biggest Loser study (Fothergill, 2016). This one is wild. They tracked the contestants 6 years later. Their resting metabolic rates were still completely tanked—burning like 500 fewer calories a day than they should be, even after they gained the weight back. The body basically holds a grudge to defend its old set point.
Also grabbed a StatPearls (2023) review and a paper by Kim (2021). The TL;DR is that for every 1% of body weight you lose, your baseline calorie burn drops. The math of “calories in, calories out” is constantly changing.
The Hormone Nightmare (Why we get so hungry):
Looked into the neurohormonal stuff (StatPearls, 2022). It’s all about the hypothalamus. When you diet, your ghrelin (hunger hormone) stays high and your leptin (satiety hormone) drops.
Klok et al. (2019) gets into the gut peptides. Your brain literally pumps out these neuropeptides (NPY and AgRP) that create an overwhelming biological drive to eat. Conscious willpower doesn’t really stand a chance against millions of years of evolution.
The Mental & Environmental Side:
Burgess (2017) and Zainal (2023) cover the psychology of it. Dieting causes chronic stress, which messes with cortisol, which leads to emotional eating. Blaming people for a “lack of discipline” totally ignores the biological stress loop.
Maffeis (2024) wrote a whole paper basically dragging the “eat less, move more” advice. They point out that weight is tied to genetics, epigenetics, and our environment. Telling someone to just eat a salad ignores the actual etiology of the problem.
Even the Drug Reviews Say It:
I pulled the clinical stakeholder input for Wegovy (Semaglutide) from CADTH (2022). Even in the official reviews for these GLP-1 drugs, the medical consensus is that just telling a patient to diet is flawed and increases psychological stigma. It’s a complex metabolic issue, not a simple math problem.
The article Lifestyle Medicine for Obesity in the Era of Highly Effective Anti-Obesity Treatment emphasizes that even with the advent of powerful anti-obesity medications, such as GLP-1 receptor agonists, lifestyle medicine remains the essential foundation of obesity care.
A comprehensive lifestyle approach—incorporating personalized nutrition, physical activity, sleep hygiene, and stress management—is crucial for maximizing the safety, efficacy, and longevity of pharmacological or surgical interventions. The discussion highlights several key clinical applications:
Mitigating Treatment Side Effects: Proper nutritional management is necessary to alleviate the gastrointestinal symptoms commonly associated with new anti-obesity medications and to prevent nutrient deficiencies during periods of significantly reduced caloric intake.
Preserving Lean Mass: Rapid weight loss often leads to the loss of muscle and bone density. Incorporating adequate dietary protein and resistance training is vital to preserve lean mass and prevent long-term complications, such as osteoporosis or sarcopenia.
Preventing Weight Regain: To attenuate metabolic adaptation and sustain weight loss over time, the authors recommend a gradual increase in physical activity, eventually targeting 200 to 300 minutes of moderate-to-vigorous exercise per week.
Multidisciplinary Delivery: Effective obesity care requires an interdisciplinary framework. Utilizing registered dietitians, shared medical appointments, and digital platforms helps clinicians deliver intensive behavioral therapy while addressing complex barriers like weight stigma, food insecurity, and psychological well-being.
Ultimately, the authors conclude that while modern pharmacotherapy offers unprecedented weight loss results, these treatments achieve their most durable and equitable outcomes when implemented alongside structured, evidence-based lifestyle modifications rather than as a standalone solution.
Sannidhi D, Abeles R, Andrew W, Bonnet JP, Vitale K, Niranjan V, Gulati M, Pauly K, Moran R, Alexander L, et al. Lifestyle Medicine for Obesity in the Era of Highly Effective Anti-Obesity Treatment. Nutrients. 2025; 17(14):2382. https://doi.org/10.3390/nu17142382
The Translation (Scripting & Flow)
This is where the magic happens. I revise the draft, translating heavy clinical speak into a conversational, high-retention script. We keep the science bulletproof but make it feel like a friendly chat.
Neuroendocrine and Socio-Environmental Determinants of Metabolic Homeostasis: The Case for Lifestyle Medicine in Obesity Management
The etiology of obesity extends significantly beyond the oversimplified thermodynamic paradigm of energy balance (calories in versus calories out). Contemporary clinical literature indicates that neuroendocrinological autonomy heavily dictates hyperphagic behaviors, often superseding conscious dietary restraint. A comprehensive review published in Nutrients elucidates the systemic impact of non-dietary lifestyle factors—specifically sleep architecture, chronic psychosocial stress, and socio-environmental determinants—on metabolic homeostasis. This multimodal approach, formally recognized as Lifestyle Medicine (LM), constitutes an evidence-based, clinically tested intervention for metabolic dysregulation.
The Synergistic Efficacy of Lifestyle Medicine Pillars
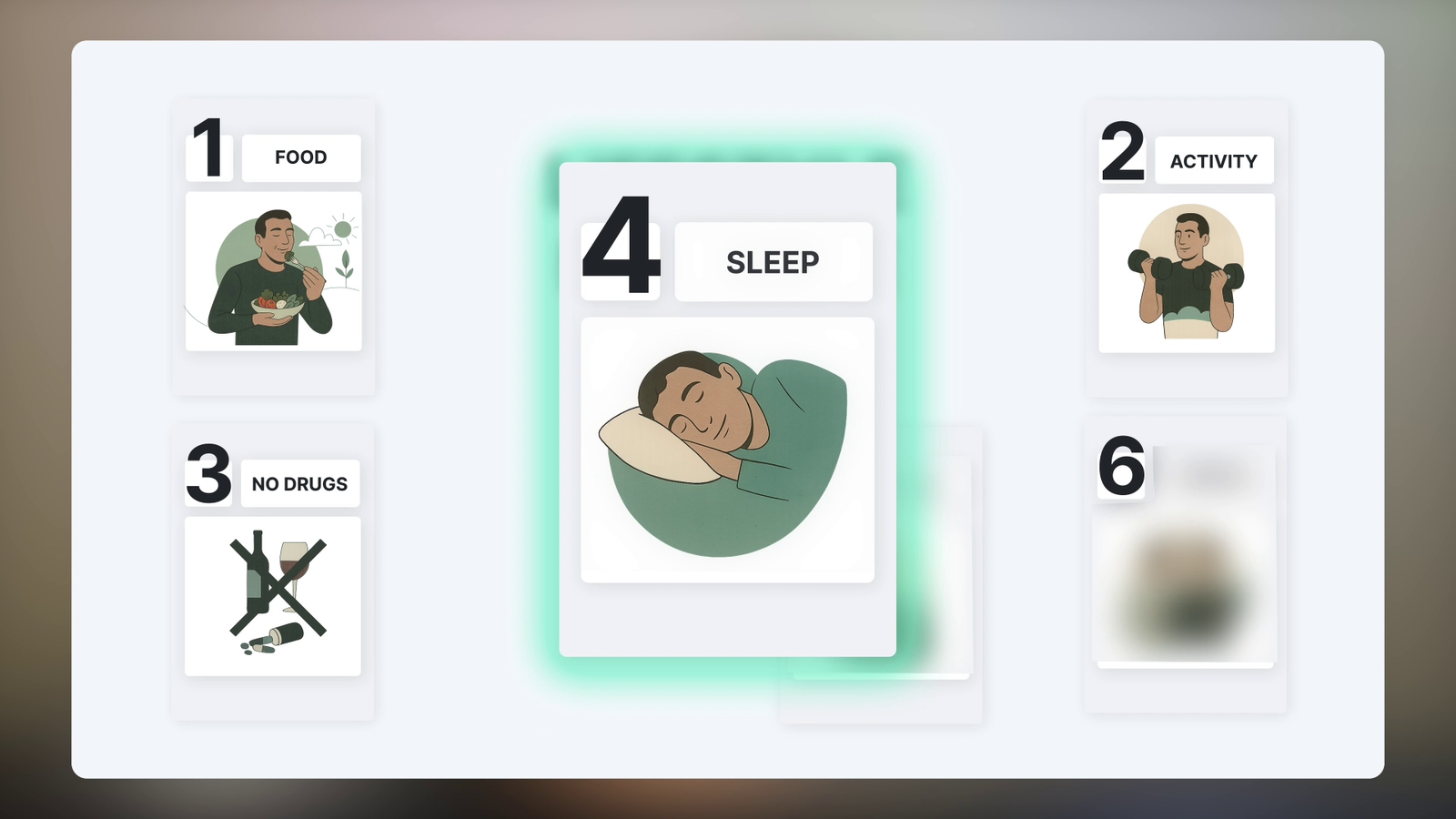
Current pharmacological and surgical interventions frequently exhibit transient efficacy due to counter-regulatory physiological adaptations upon cessation. Conversely, LM interventions target the foundational pathophysiology of metabolic syndrome via six fundamental pillars: whole-food, plant-predominant nutrition; regular physical activity; cessation of risky substance use; restorative sleep; stress management; and positive social connections.
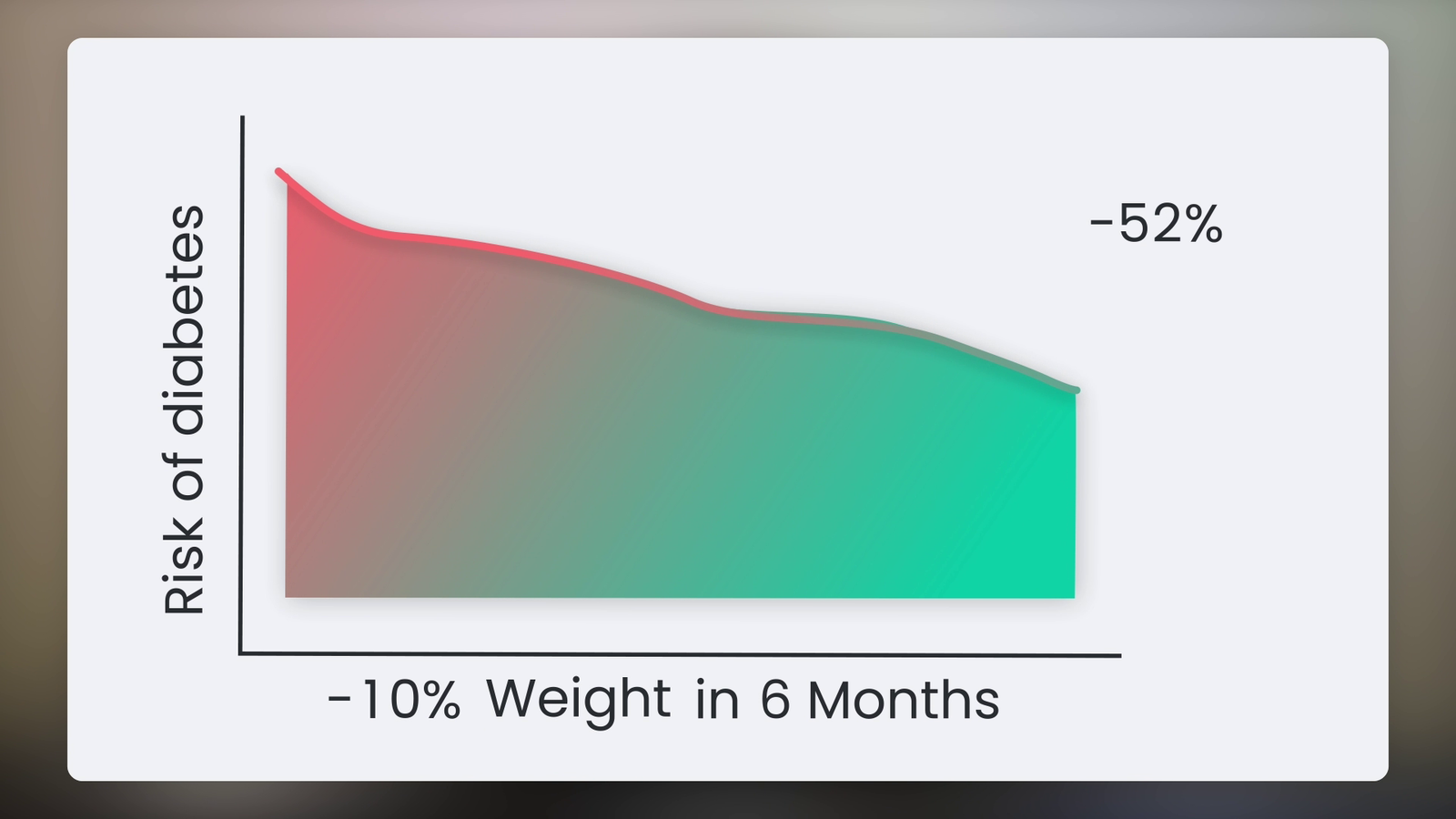
The concurrent optimization of these six domains generates a synergistic, rather than merely additive, attenuation of metabolic dysfunction. Clinical efficacy is evidenced by a standard 5% to 10% reduction in baseline body mass within a six-month interventional window. While seemingly modest, this magnitude of weight reduction yields clinically profound improvements, including a near 60% relative risk reduction in type 2 diabetes mellitus pathogenesis and substantial mitigation of cardiovascular morbidity.
Neurohormonal Dysregulation via Sleep Deprivation
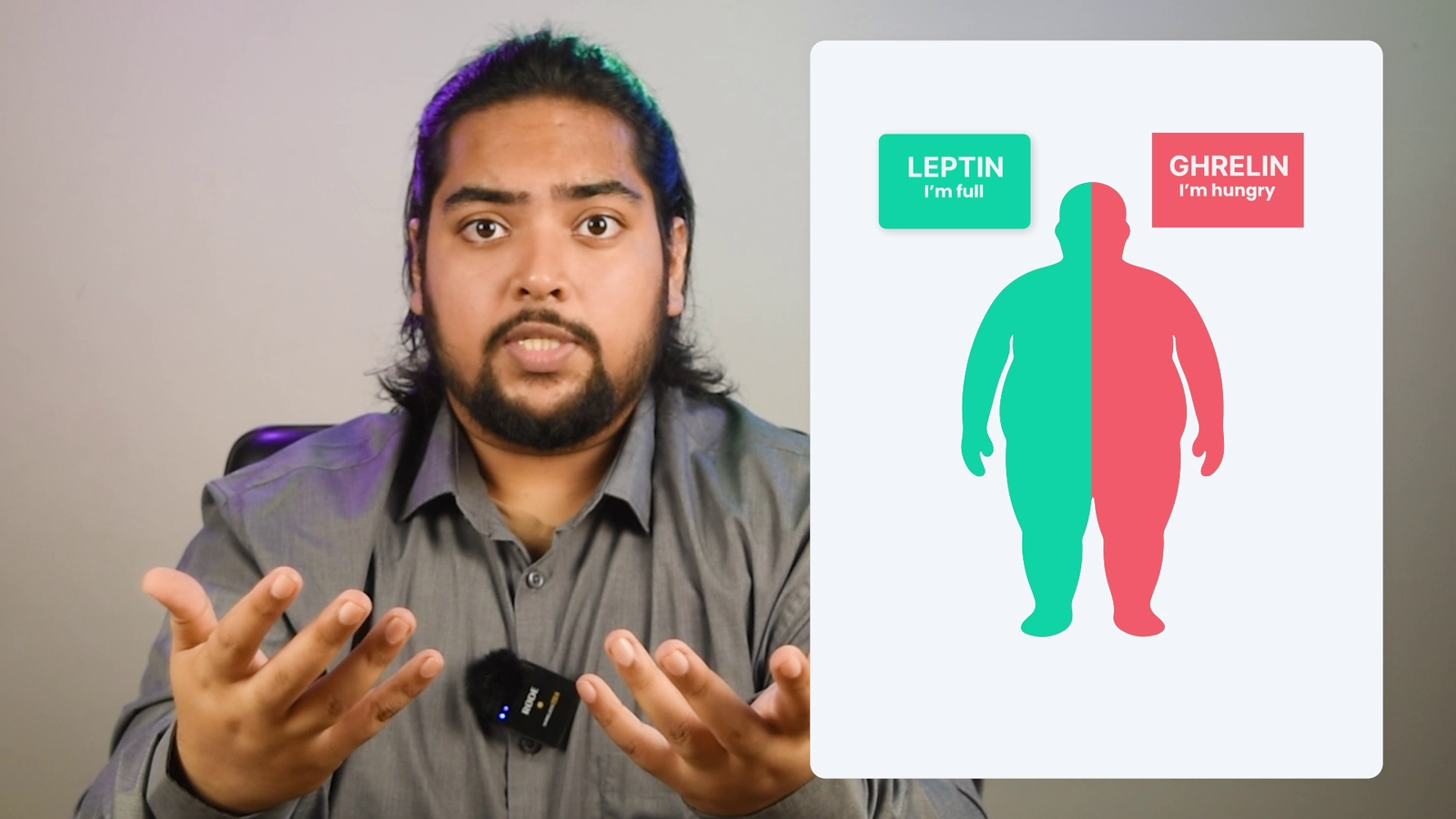
Dietary interventions are frequently undermined by unrecognized physiological barriers, primarily sleep deprivation. Suboptimal sleep duration (<6 hours per night) severely disrupts neurohormonal appetite regulation. Acute sleep deficit reliably induces an upregulation of orexigenic peptides, notably ghrelin, while simultaneously suppressing anorexigenic signaling via decreased leptin secretion. This altered neuroendocrine milieu aggressively promotes hyperphagia and a predilection for calorically dense, hyper-palatable foods, driven by biology rather than an absence of psychological willpower.
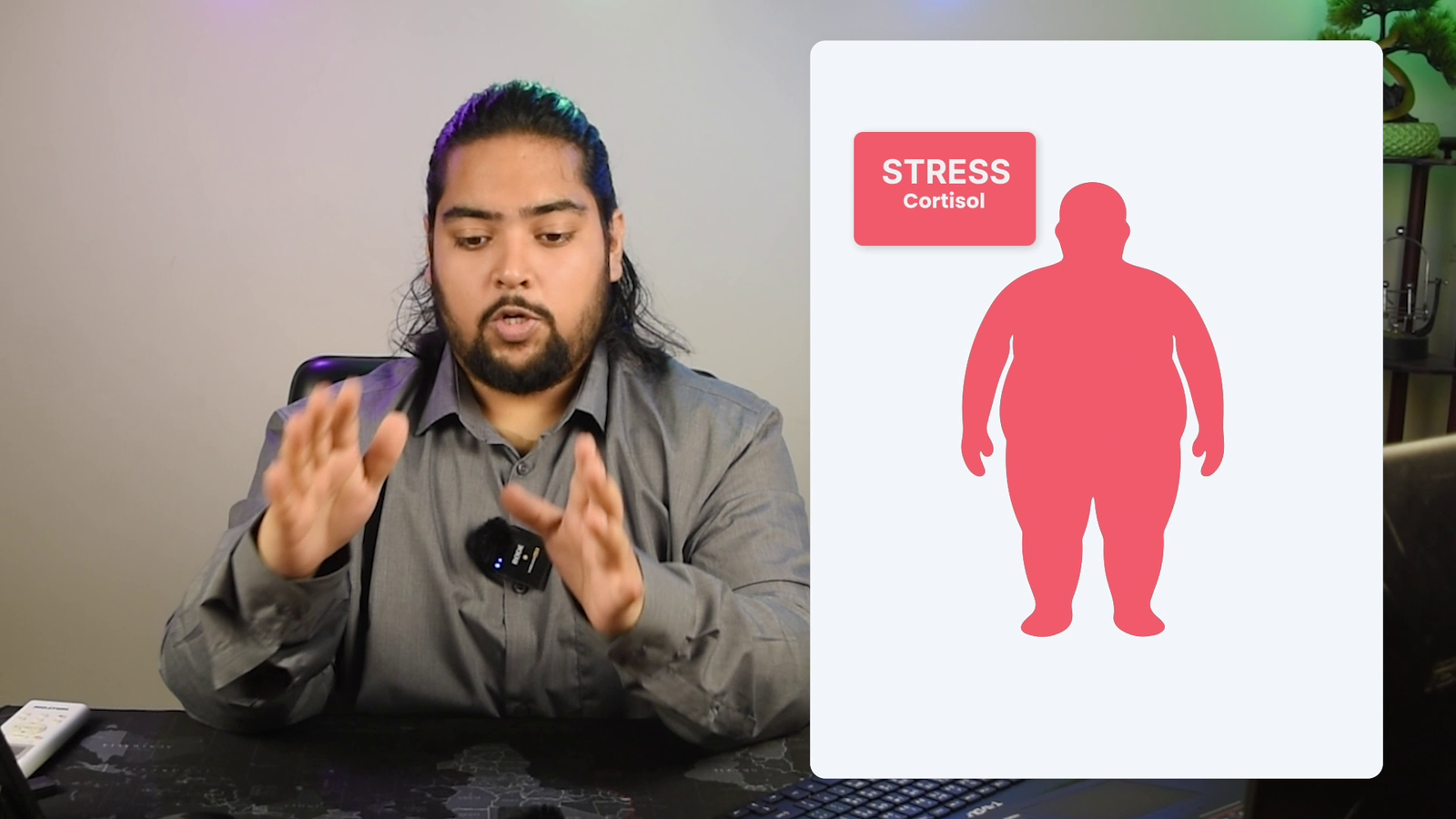
HPA-Axis Hyperactivity and Visceral Adiposity
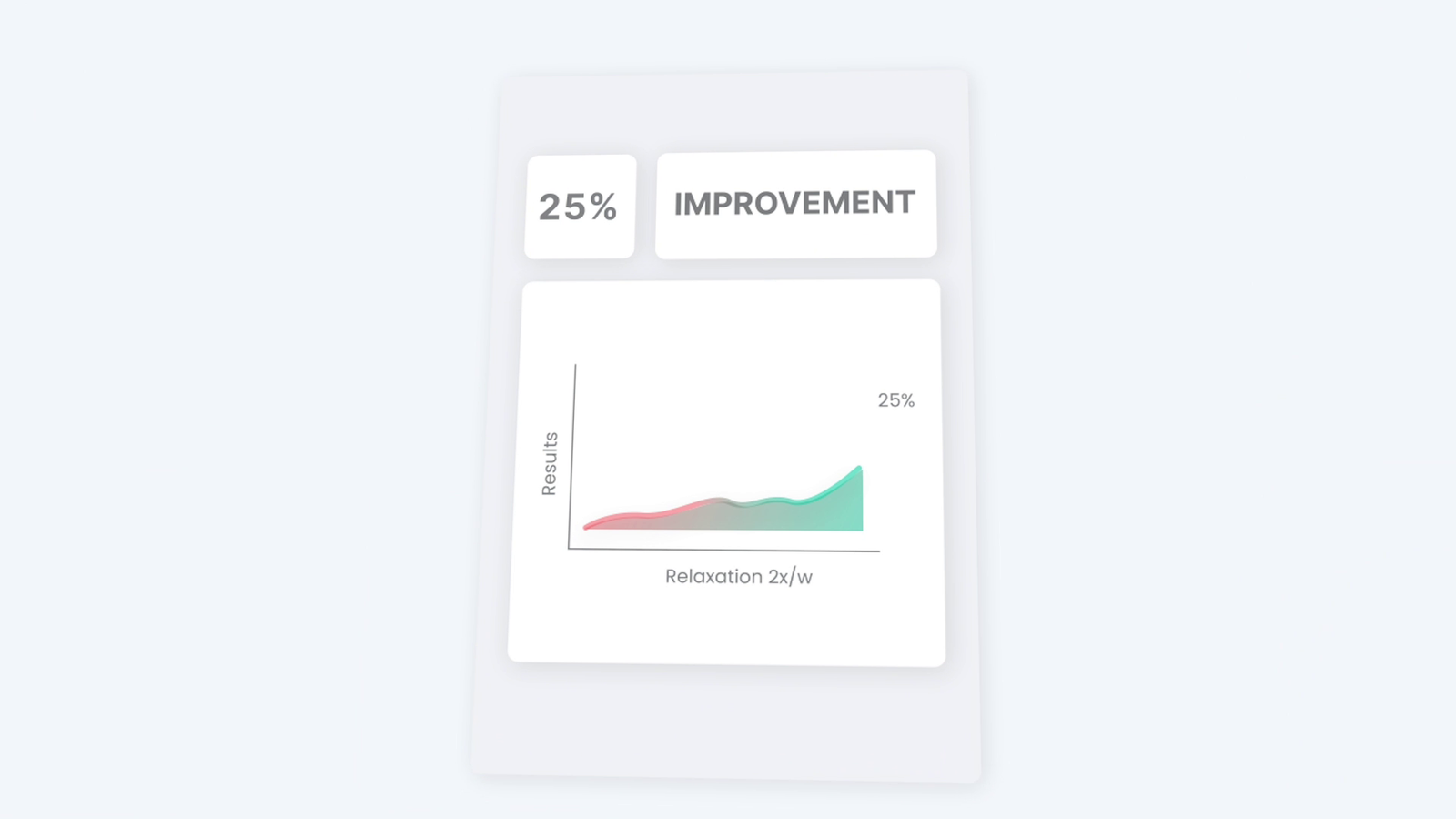
Similarly, chronic psychosocial stress acts as a primary barrier to weight reduction. Sustained psychological stress induces hyperactivity of the hypothalamic-pituitary-adrenal (HPA) axis and the sympathetic nervous system. The resultant hypercortisolemia directly facilitates the accumulation of visceral adiposity and exacerbates insulin resistance. Clinical trials indicate that integrating mindfulness-based stress reduction (MBSR) or autonomic relaxation modalities biweekly can enhance metabolic treatment outcomes by up to 25%, effectively downregulating the obesogenic “fight or flight” physiological state.
Socio-Environmental Modulation of Behavioral Adherence
Socio-environmental determinants play an underappreciated, yet critical, role in long-term weight maintenance. The prevailing literature demonstrates that cohorts engaged in structured social support systems or community-based accountability frameworks exhibit a two-to threefold increased probability of sustained weight reduction. The salutogenic or obesogenic nature of a patient’s immediate social network profoundly modulates behavioral adherence, highlighting the necessity of environmental modification in clinical treatment plans.
Clinical Implications
Singular dietary restrictions are insufficient to combat the multifactorial etiology of obesity. The authors of the Nutrients review designate Lifestyle Medicine as the “missing clinical link” in obesity treatment. The prevailing clinical consensus strongly advocates for the integration of prescription-grade LM programs into standard therapeutic protocols and insurance reimbursement frameworks, transitioning patient care from isolated symptom management to holistic physiological rehabilitation.
Why “Eat Less, Move More” is Actually Terrible Advice
Have you ever felt like your body is secretly working against your diet? Like no matter how much willpower you have, biology just takes over and forces you to the fridge at 11 PM?
For years, we’ve been told that weight loss is a simple math problem: calories in, calories out. Just eat less and move more. But if it were really that simple, we’d all have figured it out by now. Trying to fix your weight by only looking at calories is like trying to fix a leaking roof by mopping the floor. You’re working exhausting hours, but you aren’t fixing the actual problem.
Recently, a massive review published by scientists in the journal Nutrients finally explained the “why” behind the struggle. It turns out, your metabolism is shaped just as much by your sleep, your stress levels, and even your social life as it is by the food on your plate.
It’s an approach called Lifestyle Medicine, and it completely changes the game.
The 6 Pillars of Real Health
The researchers highlighted six areas we need to focus on. You already know the first three: eat whole foods, move your body, and avoid toxic substances.
But it’s the other three, the ones we usually ignore, that actually sabotage our progress.
1. The Sleep Trap
When you sleep less than six hours a night, your hunger hormones go absolutely haywire. A hormone called ghrelin (which makes you hungry) spikes, while leptin (which tells your brain you are full) crashes.
When you find yourself raiding the pantry because you are exhausted, that isn’t a lack of discipline. That is your biology doing exactly what it was programmed to do to keep you awake.
2. The Stress Belly
We tend to accept chronic stress as just a normal part of life. But when you are constantly stressed, your body gets stuck in “fight or flight” mode, flooding your system with cortisol. Cortisol is a hormone that loves to store belly fat.
The researchers found that when people simply practiced relaxing or breathing exercises a couple of times a week, their weight loss results improved by up to 25%. Relaxing is literally a weight-loss strategy.
3. Your Social Circle
This is the most underrated pillar of all. People who have a supportive community, whether that’s an online group, a workout buddy, or family members cheering them on, are two to three times more likely to keep the weight off long-term.
If everyone around you is ordering pizza, it takes a massive amount of willpower to order a salad. But if you surround yourself with people moving in the same direction, making the healthy choice suddenly feels natural.
The Missing Link
I’ve tried almost every diet out there, keto, fasting, low-calorie. They all work for a little while, but the weight always comes back because the underlying system was broken.
Medications and strict diets only work as long as you are actively on them. Lifestyle medicine actually rebuilds the foundation of how your body works so your weight can stay stable for life.
The biggest takeaway here is that you can’t medicate or diet your way out of a stressful, exhausted lifestyle. But if you start treating things like getting 8 hours of sleep, taking time to breathe, and hanging out with supportive people as actual, literal prescriptions, that is when your life actually transforms.
The “Biology vs. Willpower” Hooks
The Puppet Master: “What if I told you that your hunger isn’t a choice, but a chemical command? Scientists are discovering that your body might be making decisions long before you even open the fridge.”
The Willpower Myth: “We’ve been told for decades that weight loss is about willpower. But what if willpower is actually the last thing you should be relying on?”
The Hunger Hijack: “Ever feel like your brain is screaming for junk food even when you aren’t actually hungry? It’s not a character flaw—it’s a biological hijack. And today, we’re looking at the research on how to take the controls back.”
The Logic Gap: “Why is it that we can be the most disciplined person at work or school, but lose all control when a box of donuts appears? The answer isn’t in your mind—it’s in your metabolism.”
The “Lifestyle Medicine” Hooks
The Prescription Habit: “Imagine walking into a doctor’s office and instead of a pill, you’re handed a prescription for a better social life and two extra hours of sleep. It sounds like wishful thinking, but according to a major new study, it might be the most effective medicine we have.”
The Missing Link: “Diets fail 95% of the time. But a team of researchers just published a review in the journal Nutrients that reveals the ‘missing link’ that makes weight loss actually stick.”
The Foundation Flip: “Most people try to lose weight by changing what’s on their plate. But what if the secret to a faster metabolism has nothing to do with food at all?”
The 6-Pillar Secret: “We all know about diet and exercise. But there are four other ‘hidden’ pillars of health that scientists say are just as important for losing weight as the gym.”
The “Social & Psychological” Hooks
The Loneliness Tax: “Can being lonely actually make you gain weight? It sounds crazy, but your social life might be the secret dial controlling your metabolic rate.”
The Friendship Factor: “If your friends order pizza, you probably will too. But the science goes deeper than that. Your community doesn’t just change your habits—it actually changes your hormones.”
The Stress Trap: “You can eat all the kale in the world, but if your cortisol is spiked, your body is programmed to hold onto every ounce of fat. Here is how stress is sabotaging your scale.”
The Environment Effect: “Your kitchen, your bedroom, and your friends are constantly ‘talking’ to your metabolism. Are they telling it to burn fat, or store it?”
The “Relatable & Personal” Hooks
The Mop and the Leak: “Trying to lose weight by just counting calories is like trying to fix a leaking roof by mopping the floor. You’re working incredibly hard, but you’re not touching the actual problem.”
The Diet Merry-Go-Round: “I’ve done Keto, fasting, and low-carb. They all worked… until they didn’t. I finally found the study that explains why the weight always comes back, and how to stop the cycle.”
The Exhaustion Raiding: “We’ve all been there—standing in front of the fridge at midnight after a long day. That’s not ‘weakness.’ That’s your biology responding to a lack of sleep. Let’s talk about the science of the midnight snack.”
The Habit Reset: “Stop trying to ‘lose weight’ and start trying to ‘build a foundation.’ Today we’re breaking down the peer-reviewed evidence on why habits beat diets every single time.”
The “Short & Punchy” Hooks
The Truth About Obesity: “Obesity isn’t a lack of effort; it’s a lack of a system. A new study in Nutrients just laid out the blueprint for that system.”
The Pill vs. The Practice: “Highly effective weight loss drugs are everywhere right now. But even the best scientists admit they are useless without one specific thing.”
The 60% Statistic: “What if a few daily habits were 60% more effective at preventing diabetes than any medical intervention? The data is in, and it’s simpler than you think.”
The Metabolic Switch: “Is your metabolism broken, or is it just waiting for the right signals? Let’s look at the six signals that flip the switch from ‘store’ to ‘burn’.”
How much control do you really have over your hunger — or is it your body making the decisions for you?
What if something else — not food not willpower — was the real reason you can’t lose weight? Can friendship or loneliness actually change your metabolism?
What if your doctor could prescribe habits instead of pills — and it actually worked?
These aren’t just interesting questions — they’re the ones scientists are finally starting to answer.
A team of researchers published a major review in Nutrients, exploring how your sleep, stress, and even social life shape your metabolism as much as what’s on your plate.
It’s called Lifestyle Medicine, and it’s not a buzzword — it’s evidence-based, clinically tested, and shockingly effective.
If you like learning the real science behind weight loss…
go ahead and subscribe.
I’m sharing my own journey here — step by step.
What actually works, what doesn’t, and why.
Like a lot of people, I used to think weight loss was just about eating less and moving more. Calories in, calories out — right?
But this study shows how far off that idea really is.
It’s like trying to fix a leaking roof by mopping the floor — you’re working hard, but not on the real problem.
Lifestyle medicine goes deeper.
It’s not about a quick fix or a trendy diet — it’s about rebuilding the whole foundation of how your body and mind work together.
The researchers talk about six main pillars of lifestyle medicine.
You’ve probably heard the first few — eating whole, minimally processed foods, moving your body regularly, and avoiding harmful substances.
Nothing new there, right?
But the other three are the ones most people overlook — getting enough sleep, managing stress, and surrounding yourself with supportive people.
And here’s the interesting part: when all six come together, they don’t just add up… they
multiply.
Each one makes the others stronger, creating a kind of chain reaction for better health.
The data’s impressive.
People who embraced lifestyle-based programs — nothing extreme, just steady — lost around 5 to 10 percent of their body weight in the first six months.
That may not sound massive, but it’s life-changing.
That small drop alone cuts the risk of diabetes by nearly 60 percent and drastically lowers heart disease risk.
Think about that — not from a pill, not from surgery, but from daily habits.
And what really stood out to me wasn’t the food or workouts — we all know that, it was the stuff most of us ignore.
Take sleep for example.
When you sleep less than six hours, your hunger hormones go wild— ghrelin spikes, and leptin — the hormone that basically makes you say I’m full — drops, as a result your body literally makes you crave junk food., like your body starts shouting, “Eat something — anything.”
You’ve probably felt it. Those nights you’re exhausted and end up raiding the fridge? That’s not a weak willpower. That’s biology doing exactly what it’s programmed to do.
Btw. You can skip the gym today, but don’t skip the like button — it’s free cardio for the channel.
And who cares about stress? life is stressful we just have to live with it, right?
But the study showed that chronic stress keeps your body stuck in “fight or flight” mode, drowning in cortisol — a hormone that loves storing belly fat.
and when participants practiced mindfulness or relaxation just twice a week, their results improved by up to 25 percent.
Just imagine that — not another diet, not another workout, just breathing and giving your body permission to calm down.
And then, there’s something we almost never think of as “treatment” — relationships and social connections, the last pillar, the most underrated of all.
The paper points out that people who have a supportive community — whether that’s group check-ins, online accountability buddies, or even family members rooting for them — are two to three times more likely to maintain their weight loss long term.
It’s not about willpower or motivation, think about it,
What makes you rise to the level of the people around you.
Your environment is constantly shaping your habits, whether you notice it or not.
If everyone around you is ordering pizza, it’s harder to order a chicken salad.
But when you surround yourself with people moving in the same direction, it suddenly feels natural to keep going.
Reading this made me rethink my own journey.
Because I’ve tried almost every diet you can imagine — low-calorie, fasting, high-protein, keto — and they all worked… for a while.
But every time I stopped, the weight came back.
And now I get it.
The problem wasn’t the diet — it was the missing system.
The authors call lifestyle medicine “the missing clinical link” in treating obesity.
Why? Because medications and surgeries only work as long as you stay on them.
Lifestyle medicine builds the foundation that keeps your weight — and your health — stable for life.
It’s backed by decades of research but finally getting medical recognition as a prescription-grade therapy. In fact, the paper pushes for insurance systems and clinics to start offering lifestyle-medicine programs as standard treatment — not just “advice
So here’s the real takeaway from this study:
You can’t medicate your way out of what your lifestyle creates — I mean you can’t fix an unhealthy lifestyle with a temporary diet. But you can transform your life
Step by step. Pillar by pillar.
For me I started by fixing my sleep. practiced mindful eating and added a bit of daily movement activity.
I also needed someone to keep me accountable.
So I built this channel for that — to share the process, stay consistent, and maybe inspire someone else along the way.
Just treat those small daily actions as if they were prescriptions — because, according to this research, that’s exactly what they are.
I’d love your support — just a like is enough to let me know this message reached you.
And if you want to keep learning about what actually works — the science, the mistakes, and the reality behind real weight loss — subscribe to stay here.
We’re figuring it out together.
Phase 3: Setting the Stage (Directing & Planning)
Shot Coding
My favorite part of the prep. Every single shot gets a specific alphanumeric code. When we move to Premiere Pro, there is no guessing—everything is perfectly sequenced.
The 3-Angle Breakdown
Nobody wants to watch a static 10-minute lecture. I split the script across three distinct camera angles to keep the visual pacing dynamic and keep the viewer’s attention locked.



Director’s Notes
I leave specific cues in the margins—when to pause for emphasis, when to lean in, or when to use a prop. It takes the pressure off you during filming and makes the delivery feel completely natural.
Phase 4: Pacing & The Visual Polish (Graphics & Sound)
Anyone can add graphics, but I design visuals to reduce cognitive load and build authority. Every aesthetic choice here was deliberate.
Dialing in the Pacing (The 5-Minute Rule)
The initial script was planned for a 7-8 minute runtime, but during the edit, I ruthlessly cut it down to a fast-paced 5 minutes. Why? Because medical content can easily become a lecture. By aggressively removing the fluff and increasing the visual pacing, we respect the viewer’s time, maximize the Average View Duration (AVD), and keep the algorithm happy.
The Aesthetic Strategy (Clean vs. Techy)
I explored a “glowing, high-tech” visual style but quickly scrapped it. Neon aesthetics feel like a bio-hacker selling supplements. Instead, I built a “Clean Medical” aesthetic anchored in the brand’s teal color palette. It feels clinical, evidence-based, and instantly establishes you as a trusted physician.
Visualizing the Science (The UI Framework)
To explain the complex metabolic pathways, I generated base assets using Sora, then built an editorial collage across Photoshop, Premiere Pro, and After Effects. The core animation style relies heavily on User Interface (UI) elements—morphing cards, pop-ups, and notifications. People are conditioned to read information from their phone screens. By serving heavy medical data on familiar digital “trays,” we make the science feel incredibly accessible to the daily user.



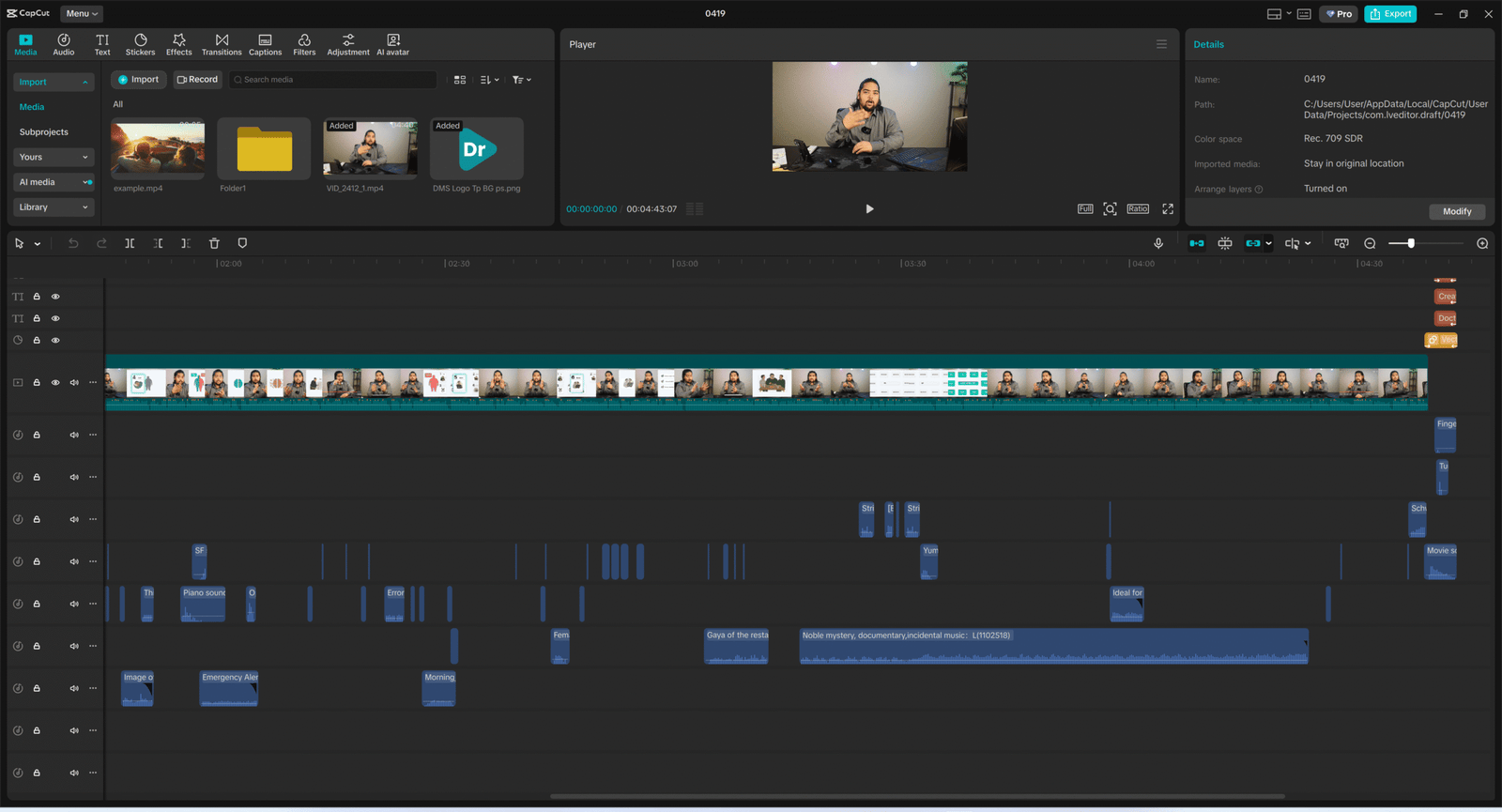
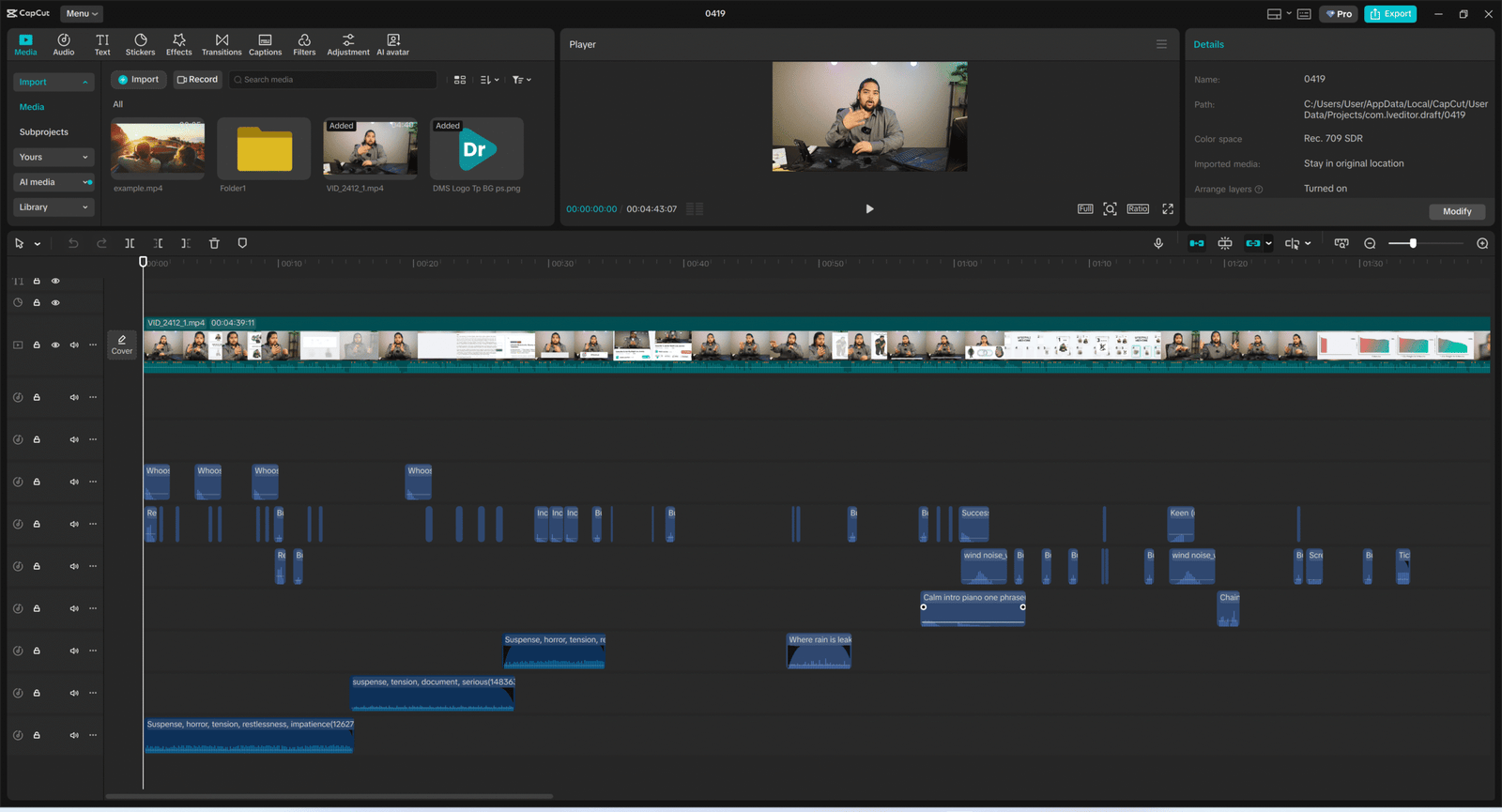
Strategic Sound Design
Audio dictates emotion. I engineered a specific audio journey: the video starts with dramatic, suspense-building tracks to hook the viewer into the “mystery” of weight loss resistance, then seamlessly transitions into an upbeat, relatable “vlog-style” sound as we reveal the actionable solutions. I utilized CapCut’s extensive commercial library for the SFX and background tracks, ensuring I get premium soundscapes with absolutely zero licensing headaches or copyright strikes down the line.
Phase 5: The Final Cut (Assembly & Handoff)
The Master Timeline
This is where the coded A-roll, the UI-style motion graphics, and the layered sound design merge into a single cohesive story. Because everything was mapped out in the scripting phase, the timeline assembly is precise and intentional, rather than a frantic search for B-roll.
The Final Handoff
The result is a highly polished, algorithm-optimized 5-minute masterclass. It is formatted and ready to be uploaded on landing page or pushed to YouTube.
Here is the final result.
Ready to Build Your Digital Clinic?
Stop letting fitness influencers control the medical narrative.
As a medical doctor, I know how frustrating it is to see bad science go viral while real clinical expertise gets buried. But as a video producer, I know exactly how to beat the algorithm at its own game.
You already have the knowledge. I provide the execution. I help clinics and health professionals translate their medical authority into high-retention, visually polished content that builds patient trust and scales your practice. You focus on the medicine; I handle the scripting, the UI animations, and the final edit.